Implanon Dosage
Generic name: etonogestrel 68mg
Dosage form: implant
Drug classes: Contraceptives, Progestogens
Medically reviewed by Drugs.com. Last updated on May 9, 2025.
The efficacy of IMPLANON does not depend on daily, weekly or monthly administration.
All healthcare providers should receive instruction and training prior to performing insertion and/or removal of IMPLANON.
A single IMPLANON implant is inserted subdermally in the upper arm. To reduce the risk of neural or vascular injury, the implant should be inserted at the inner side of the non-dominant upper arm about 8-10 cm (3-4 inches) above the medial epicondyle of the humerus. The implant should be inserted subdermally just under the skin, avoiding the sulcus (groove) between the biceps and triceps muscles and the large blood vessels and nerves that lie there in the neurovascular bundle deeper in the subcutaneous tissues. An implant inserted more deeply than subdermally (deep insertion) may not be palpable and the localization and/or removal can be difficult or impossible. IMPLANON must be inserted by the expiration date stated on the packaging. IMPLANON is a long-acting (up to 3 years), reversible, hormonal contraceptive method. The implant must be removed by the end of the third year and may be replaced by a new implant at the time of removal, if continued contraceptive protection is desired.
Initiating Contraception with IMPLANON
IMPORTANT: Rule out pregnancy before inserting the implant.
Timing of insertion depends on the woman's recent contraceptive history, as follows:
- No preceding hormonal contraceptive use in the past month
- IMPLANON should be inserted between Day 1 (first day of menstrual bleeding) and Day 5 of the menstrual cycle, even if the woman is still bleeding.
- If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
- Switching contraceptive method to IMPLANON
- Combination hormonal contraceptives:
IMPLANON should preferably be inserted on the day after the last active tablet of the previous combined oral contraceptive or on the day of the removal of the vaginal ring or transdermal patch. At the latest, IMPLANON should be inserted on the day following the usual tablet-free, ring-free, patch-free or placebo tablet interval of the previous combined hormonal contraceptive.
If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
- Progestin-only contraceptives:
There are several types of progestin-only methods. IMPLANON should be inserted as follows:
- Injectable Contraceptives: Insert IMPLANON on the day the next injection is due.
- Minipill: A woman may switch to IMPLANON on any day of the month. IMPLANON should be inserted within 24 hours after taking the last tablet.
- Contraceptive implant or intrauterine system (IUS): Insert IMPLANON on the same day as the previous contraceptive implant or IUS is removed.
If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded. - Injectable Contraceptives: Insert IMPLANON on the day the next injection is due.
- Following abortion or miscarriage
- First Trimester: IMPLANON should be inserted within 5 days following a first trimester abortion or miscarriage.
- Second Trimester: Insert IMPLANON between 21 to 28 days following second trimester abortion or miscarriage.
If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded. - First Trimester: IMPLANON should be inserted within 5 days following a first trimester abortion or miscarriage.
- Postpartum
- Not Breastfeeding: IMPLANON should be inserted between 21 to 28 days postpartum. If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
- Breastfeeding: IMPLANON should not be inserted until after the fourth postpartum week. The woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
- Not Breastfeeding: IMPLANON should be inserted between 21 to 28 days postpartum. If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
Insertion of IMPLANON
The basis for successful use and subsequent removal of IMPLANON is a correct and carefully performed subdermal insertion of the single, rod-shaped implant in accordance with the instructions. Both the healthcare provider and the woman should be able to feel the implant under the skin after placement.
All healthcare providers performing insertions and/or removals of IMPLANON should receive instructions and training prior to inserting or removing the implant. Information concerning the insertion and removal of IMPLANON will be sent upon request free of charge [1-877-IMPLANON (1-877-467-5266)].
Preparation
Prior to inserting IMPLANON carefully read the instructions for insertion as well as the full prescribing information.
Before insertion of IMPLANON, the healthcare provider should confirm that:
- The woman is not pregnant nor has any other contraindication for the use of IMPLANON.
- The woman has had a medical history and physical examination, including a gynecologic examination, performed.
- The woman understands the benefits and risks of IMPLANON.
- The woman has received a copy of the Patient Labeling included in packaging.
- The woman has reviewed and completed a consent form to be maintained with the woman's chart.
- The woman does not have allergies to the antiseptic and anesthetic to be used during insertion.
Insert IMPLANON under aseptic conditions.
The following equipment is needed for the implant insertion:
- An examination table for the woman to lie on
- Sterile surgical drapes, sterile gloves, antiseptic solution, sterile marker (optional)
- Local anesthetic, needles, and syringe
- Sterile gauze, adhesive bandage, pressure bandage
An applicator and its parts are shown below (Figures 1a and 1b).
| Figure 1a (Not to scale) |
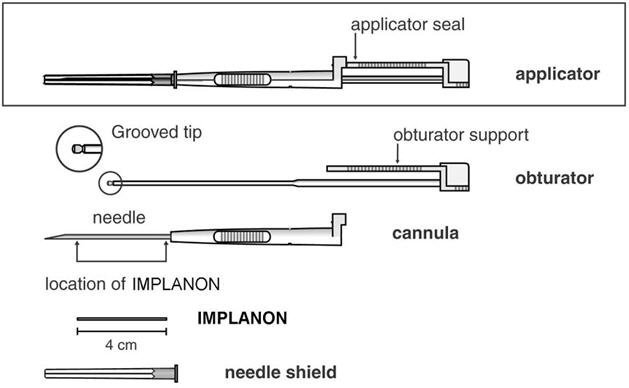 |
| Figure 1b |
 |
| Grooved tip of obturator (enlarged) |
The procedure used for IMPLANON insertion is opposite from that of an injection. The obturator keeps IMPLANON in place while the cannula is retracted. The obturator must remain fixed in place while the cannula with needle is retracted from the arm. Do not push the obturator.
Insertion Procedure
- Step 1. Have the woman lie on her back on the examination table with her non-dominant arm flexed at the elbow and externally rotated so that her wrist is parallel to her ear or her hand is positioned next to her head (Figure 2).

-
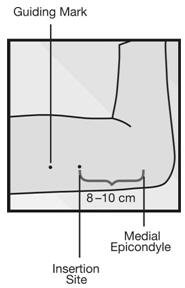
Step 2. Identify the insertion site, which is at the inner side of the non-dominant upper arm about 8-10 cm (3-4 inches) above the medial epicondyle of the humerus, avoiding the sulcus (groove) between the biceps and triceps muscles and the large blood vessels and nerves that lie there in the neurovascular bundle deeper in the subcutaneous tissue (Figure 3). The implant should be inserted subdermally just under the skin.
- Step 3. Make two marks with a sterile marker: first, mark the spot where the etonogestrel implant will be inserted, and second, mark a spot a few centimeters proximal to the first mark (Figure 3). This second mark will later serve as a direction guide during insertion.
- Step 4. Clean the insertion site with an antiseptic solution.
- Step 5. Anesthetize the insertion area (for example, with anesthetic spray or by injecting 2 mL of 1% lidocaine just under the skin along the planned insertion tunnel).
- Step 6. Remove the sterile pre-loaded disposable IMPLANON applicator carrying the implant from its blister. Keep the IMPLANON needle and rod sterile. The applicator should not be used if sterility is in question. If contamination occurs, use a new package of IMPLANON with a new sterile applicator.
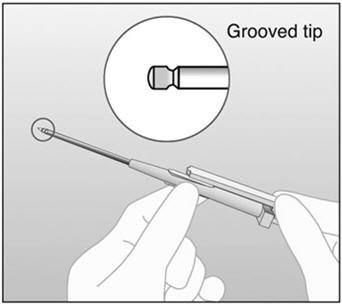
- Step 7. Keep the shield on the needle and look for the IMPLANON rod, seen as a white cylinder inside the needle tip.
- Step 8. If you don't see the IMPLANON rod, tap the top of the needle shield against a firm surface to bring the implant into the needle tip.
- Step 9. Following visual confirmation, lower the IMPLANON rod back into the needle by tapping it back into the needle tip. Then remove the needle shield, while holding the applicator upright.
- Step 10. Note that IMPLANON can fall out of the needle. Therefore, after you remove the needle shield, keep the applicator in the upright position until the moment of insertion
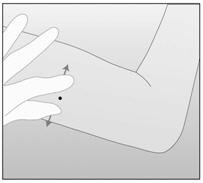
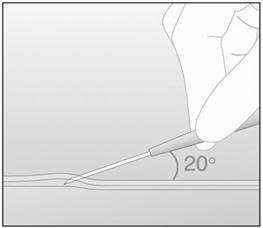
- Step 11. With your free hand, stretch the skin around the insertion site with thumb and index finger (Figure 4).
- Step 12. At a slight angle (not greater than 20°), insert only the tip of the needle with the beveled side up into the insertion site (Figure 5).
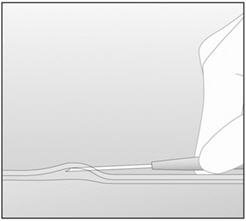
- Step 13. Lower the applicator to a horizontal position. Lift the skin up with the tip of the needle, but keep the needle in the subdermal connective tissue (Figure 6).
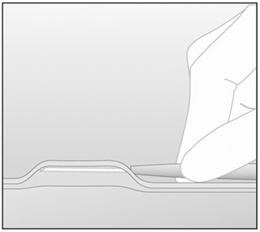
- Step 14. While "tenting" (lifting) the skin, gently insert the needle to its full length. Keep the needle parallel to the surface of the skin during insertion (Figure 7).
-
Step 15. If IMPLANON is placed deeply, the removal process can be difficult or impossible. If the needle is not inserted to its full length, the implant may protrude from the insertion site and fall out.
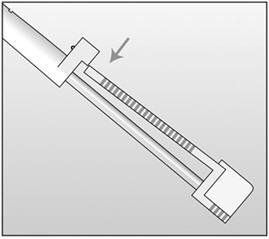
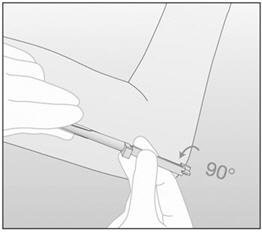
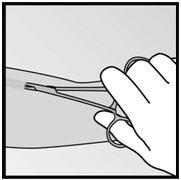
- Step 16. Break the seal of the applicator by pressing the obturator support (Figure 8).
- Step 17. Turn the obturator 90° in either direction with respect to the needle (Figure 9).
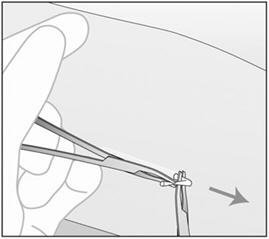
- Step 18. While holding the obturator fixed in place on the arm, fully retract the cannula (Figure 10). Note: This procedure is opposite from an injection. Do not push the obturator. By holding the obturator fixed in place on the arm and fully retracting the cannula, the implant will be left in its correct subdermal position. Do not simultaneously retract the obturator and cannula from the patient's arm.
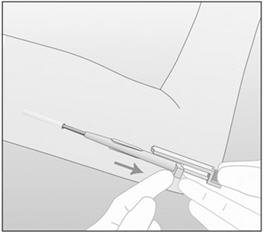 |
| Figure 10 |
| In this figure, the right hand is holding the obturator in place while the left hand is retracting the cannula. |
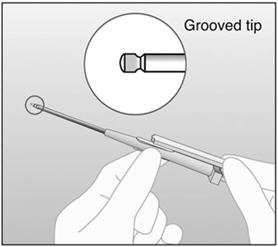
- Step 19. Confirm that the implant has been inserted by checking the tip of the needle for the absence of the implant. After insertion of the implant, the grooved tip of the obturator will be visible inside the needle (Figure 11).
-
Step 20. Always verify the presence of the implant in the woman's arm immediately after insertion by palpation. By palpating both ends of the implant, you should be able to confirm the presence of the 4-cm rod (Figure 12). See section below "If the rod is not palpable".

-
Step 21. Place a small adhesive bandage over the insertion site. Request that the woman palpate the implant.
-
Step 22. Apply a pressure bandage with sterile gauze to minimize bruising. The woman may remove the pressure bandage in 24 hours and the small bandage over the insertion site in 3 to 5 days.
-
Step 23. Complete the USER CARD and give it to the woman to keep. Also, complete the PATIENT CHART LABEL and affix it to the woman's medical record.
-
Step 24. The applicator is for single use only and should be disposed in accordance with the Center for Disease Control and Prevention guidelines for handling of hazardous waste.
If you cannot feel the implant or are in doubt of its presence, the implant may not have been inserted or it may have been inserted deeply:
- Check the tip of the needle for the absence of the implant. After insertion of the implant, the grooved tip of the obturator will be visible inside the needle.
- Use other methods to confirm the presence of the implant. Suitable methods to locate are: ultrasound (US) with a high-frequency linear array transducer (10 MHz or greater) or magnetic resonance imaging (MRI). Please note that the IMPLANON rod is not radiopaque and cannot be seen by X-ray or CT scan. If ultrasound and MRI fail, call 1-877-IMPLANON (1-877-467-5266) for information on the procedure for measuring etonogestrel blood levels.
Until the presence of the implant has been verified, the woman should be advised to use a non-hormonal contraceptive method, such as condoms.
Once the non-palpable implant has been located, removal is recommended.
Removal of IMPLANON
Preparation
Before initiating the removal procedure, the healthcare provider should carefully read the instructions for removal and consult the USER CARD and/or the PATIENT CHART LABEL for the location of the implant. The exact location of the implant in the arm should be verified by palpation.
Procedure for Removal of an Implant that is Palpable
Before removal of the implant, the healthcare provider should confirm that:
- The woman does not have allergies to the antiseptic or anesthetic to be used.
Remove the implant under aseptic conditions.
The following equipment is needed for removal of the implant:
- An examination table for the woman to lie on
- Sterile surgical drapes, sterile gloves, antiseptic solution, sterile marker (optional)
- Local anesthetic, needles, and syringe
- Sterile scalpel, forceps (straight and curved mosquito)
- Skin closure, sterile gauze, adhesive bandage and pressure bandages
Removal Procedure
- Step 1. Clean the site where the incision will be made and apply an antiseptic. Locate the implant by palpation and mark the distal end (end closest to the elbow), for example, with a sterile marker (Figure 13).
- Step 2. Anesthetize the arm, for example, with 0.5 to 1 mL 1% lidocaine at the marked site where the incision will be made (Figure 14). Be sure to inject the local anesthetic under the implant to keep it close to the skin surface.

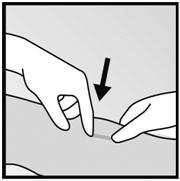
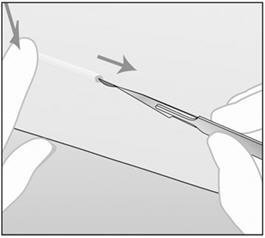
- Step 3. Push down the proximal end of the implant (Figure 15) to stabilize it; a bulge may appear indicating the distal end of the implant. Starting at the distal tip of the implant, make a longitudinal incision of 2 mm towards the elbow.
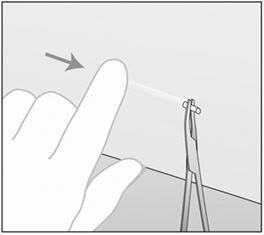
- Step 4. Gently push the implant towards the incision until the tip is visible. Grasp the implant with forceps (preferably curved mosquito forceps) and gently remove the implant (Figure 16).
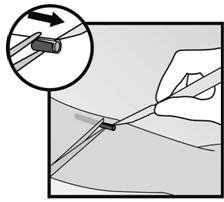
- Step 5. If the implant is encapsulated, make an incision into the tissue sheath and then remove the implant with the forceps (Figures 17 and 18).
 |
 |
| Figure 17 | Figure 18 |
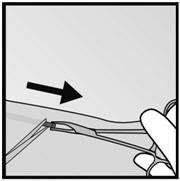
- Step 6. If the tip of the implant does not become visible in the incision, gently insert a forceps into the incision (Figure 19). Flip the forceps over into your other hand (Figure 20).
 |
 |
| Figure 19 | Figure 20 |
- Step 7. With a second pair of forceps carefully dissect the tissue around the implant and grasp the implant (Figure 21). The implant can then be removed.
-
Step 8. Confirm that the entire implant, which is 4 cm long, has been removed by measuring its length. There have been reports of broken implants while in the patient's arm. In some cases, difficult removal of the broken implant has been reported. If a partial implant (less than 4 cm) is removed, the remaining piece should be removed by following the instructions in section 2.3. If the woman would like to continue using IMPLANON, a new implant may be inserted immediately after the old implant is removed using the same incision.
- Step 9. After removing the implant, close the incision with a steri-strip and apply an adhesive bandage.
- Step 10. Apply a pressure bandage with sterile gauze to minimize bruising. The woman may remove the pressure bandage in 24 hours and the small bandage in 3 to 5 days.
Localization and Removal of a Non-Palpable Implant
There have been reports of migration of the implant; usually this involves minor movement relative to the original position, but may lead to the implant not being palpable in the location in which it was placed. An implant that has been deeply inserted or has migrated may not be palpable and therefore imaging procedures, as described below, may be required for localization.
A non-palpable implant should always be located prior to attempting removal. Suitable methods for localization include ultrasound with a high-frequency linear array transducer (10 MHz or greater) or magnetic resonance imaging. Once the implant has been localized in the arm, the implant should be removed according to the instructions in Dosage and Administration (2.3), Procedure for Removal of an Implant that is Palpable, and the use of ultrasound guidance during the removal should be considered.
If the implant cannot be found in the arm after comprehensive localization attempts, consult a radiologist familiar with applying advanced imaging techniques to the chest, as events of migration to the pulmonary vasculature have been reported. If the implant is located in the chest, surgical or endovascular procedures may be needed for removal; healthcare providers familiar with the anatomy of the chest should be consulted.
If at any time these imaging methods fail to locate the implant, etonogestrel blood level determination can be used for verification of the presence of the implant. For details on etonogestrel blood level determination, call 1-877-IMPLANON (1-877-467-5266) for further instructions.
If the implant migrates within the arm, removal may require a minor surgical procedure with a larger incision or a surgical procedure in an operating room. Removal of deeply inserted implants should be conducted with caution in order to prevent injury to deeper neural or vascular structures in the arm and be performed by healthcare providers familiar with the anatomy of the arm.
Exploratory surgery without knowledge of the exact location of the implant is strongly discouraged.
Replacing IMPLANON
Immediate replacement can be done after removal of the previous implant and is similar to the insertion procedure described in section 2.2 Insertion of IMPLANON.
The new implant may be inserted in the same arm, and through the same incision from which the previous implant was removed. If the same incision is being used to insert a new implant, anesthetize the insertion site [for example, 2 mL lidocaine (1%)] applying it just under the skin along the 'insertion canal.'
Follow the subsequent steps in the insertion instructions.
Frequently asked questions
- When will I get my first period after inserting the Implanon implant?
- What is the difference between Nexplanon and Implanon?
More about Implanon (etonogestrel)
- Check interactions
- Compare alternatives
- Reviews (1,684)
- Side effects
- During pregnancy
- Support group
- FDA approval history
- Drug class: contraceptives
- Breastfeeding
Patient resources
Other brands
Professional resources
Other brands
Related treatment guides
See also:
Further information
Always consult your healthcare provider to ensure the information displayed on this page applies to your personal circumstances.
