Nicotrol Inhalant: Package Insert / Prescribing Info
Package insert / product label
Generic name: nicotine
Dosage form: inhalation system
Drug class: Smoking cessation agents
Medically reviewed by Drugs.com. Last updated on Mar 25, 2025.
On This Page
- Description
- Clinical Pharmacology
- Clinical Studies
- Indications and Usage
- Contraindications
- Warnings
- Precautions
- Patient Counseling Information
- Drug Interactions
- Adverse Reactions/Side Effects
- Drug Abuse and Dependence
- Overdosage
- Dosage and Administration
- Storage and Handling
- How Supplied/Storage and Handling
Nicotrol Inhalant Description
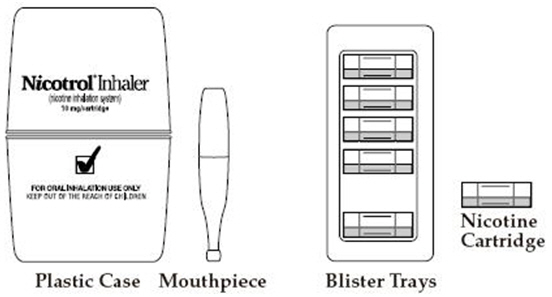
NICOTROL® Inhaler (nicotine inhalation system) consists of a mouthpiece and a plastic cartridge delivering 4 mg of nicotine from a porous plug containing 10 mg nicotine. The cartridge is inserted into the mouthpiece prior to use. Nicotine is a tertiary amine composed of a pyridine and a pyrrolidine ring. It is a colorless to pale yellow, freely water-soluble, strongly alkaline, oily, volatile, hygroscopic liquid obtained from the tobacco plant. Nicotine has a characteristic pungent odor and turns brown on exposure to air or light. Of its two stereoisomers, S(-)nicotine is the more active. It is the prevalent form in tobacco and is the form in the NICOTROL Inhaler. The free alkaloid is absorbed rapidly through skin, mucous membranes, and the respiratory tract.
Chemical Name: S-3-(1-methyl-2-pyrrolidinyl) pyridine
Molecular Formula: C10H14N2
Molecular Weight: 162.23
Ionization Constants: pKa1 = 7.84, pKa2 = 3.04 at 15°C
Octanol-Water Partition Coefficient: 15:1 at pH 7
Nicotine is the active ingredient; inactive components of the product are menthol and a porous plug which are pharmacologically inactive. Nicotine is released when air is inhaled through the inhaler.
Nicotrol Inhalant - Clinical Pharmacology
Pharmacologic Action
Nicotine, the chief alkaloid in tobacco products, binds stereo-selectively to nicotinic-cholinergic receptors at the autonomic ganglia, in the adrenal medulla, at neuromuscular junctions, and in the brain. Two types of central nervous system effects are believed to be the basis of nicotine's positively reinforcing properties. A stimulating effect is exerted mainly in the cortex via the locus ceruleus and a reward effect is exerted in the limbic system. At low doses the stimulant effects predominate while at high doses the reward effects predominate. Intermittent intravenous administration of nicotine activates neurohormonal pathways, releasing acetylcholine, norepinephrine, dopamine, serotonin, vasopressin, beta-endorphin, growth hormone, and ACTH.
Pharmacodynamics
The cardiovascular effects of nicotine include peripheral vasoconstriction, tachycardia, and elevated blood pressure. Acute and chronic tolerance to nicotine develops from smoking tobacco or ingesting nicotine preparations. Acute tolerance (a reduction in response for a given dose) develops rapidly (less than 1 hour), but not at the same rate for different physiologic effects (skin temperature, heart rate, subjective effects). Withdrawal symptoms such as cigarette craving can be reduced in most individuals by plasma nicotine levels lower than those from smoking.
Withdrawal from nicotine in addicted individuals can be characterized by craving, nervousness, restlessness, irritability, mood lability, anxiety, drowsiness, sleep disturbances, impaired concentration, increased appetite, minor somatic complaints (headache, myalgia, constipation, fatigue), and weight gain. Nicotine toxicity is characterized by nausea, abdominal pain, vomiting, diarrhea, diaphoresis, flushing, dizziness, disturbed hearing and vision, confusion, weakness, palpitations, altered respiration and hypotension.
Both smoking and nicotine can increase circulating cortisol and catecholamines, and tolerance does not develop to the catecholamine-releasing effects of nicotine. Changes in the response to a concomitantly administered adrenergic agonist or antagonist should be watched for when nicotine intake is altered during NICOTROL Inhaler therapy and/or smoking cessation (See PRECAUTIONS, Drug Interactions).
Pharmacokinetics
Absorption
Most of the nicotine released from the NICOTROL Inhaler is deposited in the mouth. Only a fraction of the dose released, less than 5%, reaches the lower respiratory tract. An intensive inhalation regimen (80 deep inhalations over 20 minutes) releases on the average 4 mg of the nicotine content of each cartridge of which about 2 mg is systemically absorbed. Peak plasma concentrations are typically reached within 15 minutes of the end of inhalation.
Absorption of nicotine through the buccal mucosa is relatively slow and the high and rapid rise followed by the decline in nicotine arterial plasma concentrations seen with cigarette smoking are not achieved with the inhaler. After use of the single inhaler the arterial nicotine concentrations rise slowly to an average of 6 ng/mL in contrast to those of a cigarette, which increase rapidly and reach a mean Cmax of approximately 49 ng/mL within 5 minutes.
The temperature dependency of nicotine release from the NICOTROL Inhaler was studied between 68°F and 104°F in eighteen patients. Average achievable steady-state plasma levels after 20 minutes of an intensive inhalation regimen each hour at ambient room temperature are on the order of 23 ng/mL. The corresponding nicotine plasma levels achievable at 86°F and 104°F are on the order of 30 and 34 ng/mL. Nicotine peak plasma concentration (Cmax) at steady-state, after 20 minutes of an intensive inhalation regimen per hour, for 10 hours.
| Cmax (ng/mL) | |||
|---|---|---|---|
| 20°C/68°F | 30°C/86°F | 40°C/104°F | |
| N=18 | N=18 | N=18 | |
|
Mean |
22.5 |
29.7 |
34.0 |
|
S.D. |
7.7 |
8.3 |
6.9 |
|
Min |
11.1 |
17.6 |
24.1 |
|
Max |
40.4 |
47.2 |
48.6 |
Ad libitum use of the NICOTROL Inhaler typically produces nicotine plasma levels of 6–8 ng/mL, corresponding to about 1/3 of those achieved with cigarette smoking.
Distribution
The volume of distribution following IV administration of nicotine is approximately 2 to 3 L/kg. Plasma protein binding of nicotine is <5%. Therefore, changes in nicotine binding from use of concomitant drugs or alterations of plasma proteins by disease states would not be expected to have significant effects on nicotine kinetics.
Metabolism
More than 20 metabolites of nicotine have been identified, all of which are less active than the parent compound. The primary urinary metabolites are cotinine (15% of the dose) and trans-3-hydroxycotinine (45% of the dose). Cotinine has a half-life of 15 to 20 hours and concentrations that exceed nicotine by 10-fold. The major site for the metabolism of nicotine is the liver. The kidney and lung are also sites of nicotine metabolism.
Elimination
About 10% of the nicotine absorbed is excreted unchanged in the urine. This may be increased to up to 30% with high urine flow rates and urinary acidification below pH 5. The average plasma clearance is about 1.2 L/min in a healthy adult smoker. The apparent elimination half-life of nicotine is 1 to 2 hours.
Gender Differences
Intersubject variability coefficients of variation (C.V.) for the pharmacokinetic parameters (AUC and Cmax) were approximately 40% and 30% respectively, for males and females. There were no medically significant differences between females and males in the kinetics of NICOTROL Inhaler.
Renal Impairment
Progressive severity of renal impairment is associated with decreased total clearance of nicotine. Nicotine clearance was decreased by 30% on average in subjects with moderate renal impairment and 50% on average in subjects with severe renal impairment.
Hepatic Impairment
In smokers with liver cirrhosis but only mild impairment of hepatic function (Child-Pugh score 5), the pharmacokinetics of nicotine is unaffected. However, in smokers with moderately impaired liver function (Child-Pugh score 7), total clearance has been reported to be reduced on average by 40–50%. There are no data about the pharmacokinetics of nicotine in smokers with a Child-Pugh score exceeding 7 but these subjects are expected to show similar or greater effects on clearance of nicotine as patients with moderately impaired liver function.
CLINICAL TRIALS
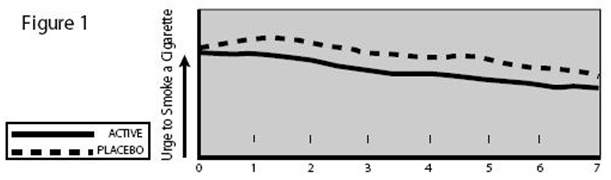
The efficacy of NICOTROL Inhaler therapy as an aid to smoking cessation was demonstrated in two single-center, placebo-controlled, double-blind trials with a total of 445 healthy patients. The number of NICOTROL Inhaler cartridges used was a minimum dose of 4 cartridges/day and a maximum dose of 20 cartridges/day. In both studies, the recommended duration of treatment was 3 months; however, the patients were permitted to continue to use the product for up to 6 months, if they wished. The quit rates are the percentage of all persons initially enrolled who continuously abstained after week 2. NICOTROL Inhaler was more effective than placebo at 6 weeks, 3 months and 6 months. The efficacy is shown in the following table.
| Quit Rates by Treatment
(N= 445 Patients in 2 Studies) |
|||||
|---|---|---|---|---|---|
| Group | Number of Patients | At 6 Weeks | At 3 Months | At 6 Months | At 12 Months* |
|
|||||
|
NICOTROL Inhaler |
223 |
44–45% |
31–32% |
20–21% |
11–13% |
|
Placebo |
222 |
14–23% |
8–15% |
6–11% |
5–10% |
Patients who used NICOTROL Inhaler had a significant reduction in the "urge to smoke", a major nicotine withdrawal symptom, compared with placebo-treated patients throughout the first week (See Figure 1).
Indications and Usage for Nicotrol Inhalant
NICOTROL Inhaler is indicated as an aid to smoking cessation for the relief of nicotine withdrawal symptoms. NICOTROL Inhaler therapy is recommended for use as part of a comprehensive behavioral smoking cessation program.
Contraindications
Use of NICOTROL Inhaler therapy is contraindicated in patients with known hypersensitivity or allergy to nicotine or to menthol.
Warnings
Nicotine from any source can be toxic and addictive. Smoking causes lung disease, cancer and heart disease, and may adversely affect pregnant women or the fetus. For any smoker, with or without concomitant disease or pregnancy, the risk of nicotine replacement in a smoking cessation program should be weighed against the hazard of continued smoking, and the likelihood of achieving cessation of smoking without nicotine replacement.
Pregnancy, Warning
Tobacco smoke, which has been shown to be harmful to the fetus, contains nicotine, hydrogen cyanide, and carbon monoxide. The NICOTROL Inhaler does not deliver hydrogen cyanide and carbon monoxide. However, nicotine has been shown in animal studies to cause fetal harm. It is therefore presumed that NICOTROL Inhaler can cause fetal harm when administered to a pregnant woman. The effect of nicotine delivery by NICOTROL Inhaler has not been examined in pregnancy (See PRECAUTIONS). Therefore, pregnant smokers should be encouraged to attempt cessation using educational and behavioral interventions before using pharmacological approaches. If NICOTROL Inhaler is used during pregnancy, or if the patient becomes pregnant while using it, the patient should be apprised of the potential hazard to the fetus.
Safety Note Concerning Children
This product contains nicotine and should be kept out of the reach of children and pets. The amounts of nicotine that are tolerated by adult smokers can produce signs and symptoms of poisoning and could prove fatal if the nicotine from the NICOTROL Inhaler is inhaled, ingested, or buccally absorbed by children or pets. Suspected nicotine poisoning in a child should be considered a medical emergency and treated immediately. A cartridge contains about 60% of its initial drug content when it is discarded, which is about 6 mg. Patients should be cautioned to keep both the used and unused cartridges of NICOTROL Inhaler out of the reach of children and pets.
All components of the NICOTROL Inhaler system should also be kept out of the reach of children and pets to avoid accidental swallowing and choking.
Precautions
General
The patient should be urged to stop smoking completely when initiating NICOTROL Inhaler therapy (See DOSAGE AND ADMINISTRATION). Patients should be informed that if they continue to smoke while using the product, they may experience adverse effects due to peak nicotine levels higher than those experienced from smoking alone. If there is a clinically significant increase in cardiovascular or other effects attributable to nicotine, the treatment should be discontinued (See WARNINGS). Physicians should anticipate that concomitant medications may need dosage adjustment (See Drug Interactions). Sustained use (beyond 6 months) of NICOTROL Inhaler by patients who stop smoking has not been studied and is not recommended. (See DRUG ABUSE AND DEPENDENCE).
Bronchospastic Disease
NICOTROL Inhaler has not been specifically studied in asthma or chronic pulmonary disease. Nicotine is an airway irritant and might cause bronchospasm. NICOTROL Inhaler should be used with caution in patients with bronchospastic disease. Other forms of nicotine replacement might be preferable in patients with severe bronchospastic airway disease.
Cardiovascular or Peripheral Vascular Diseases
The risks of nicotine replacement in patients with cardiovascular and peripheral vascular diseases should be weighed against the benefits of including nicotine replacement in a smoking cessation program for them. Specifically, patients with coronary heart disease (history of myocardial infarction and/or angina pectoris), serious cardiac arrhythmias, or vasospastic diseases (Buerger's disease, Prinzmetal's variant angina and Raynaud's phenomena) should be evaluated carefully before nicotine replacement is prescribed.
Tachycardia and palpitations have been reported occasionally with the use of NICOTROL Inhaler as well as with other nicotine replacement therapies. No serious cardiovascular events were reported in clinical studies with NICOTROL Inhaler, but if such symptoms occur, its use should be discontinued.
NICOTROL Inhaler generally should not be used in patients during the immediate post-myocardial infarction period, nor in patients with serious arrhythmias, or with severe or worsening angina.
Renal or Hepatic Insufficiency
Pharmacokinetic studies in patients with moderate to severe renal impairment or moderate to severe hepatic impairment have shown decreased nicotine clearance. The pharmacokinetics of nicotine have not been studied in the elderly. Given that nicotine is extensively metabolized and that its total system clearance is dependent on liver blood flow, some influence of hepatic impairment on drug kinetics (reduced clearance with potential for increased adverse effects) are anticipated. Moderate and severe renal impairment are expected to affect the clearance of nicotine or its metabolites from the circulation (See PHARMACOKINETICS). Consider dose reduction and monitoring patients for adverse events (such as nausea or dizziness) associated with elevated levels of nicotine.
Endocrine Diseases
NICOTROL Inhaler therapy should be used with caution in patients with hyperthyroidism, pheochromocytoma or insulin-dependent diabetes since nicotine causes the release of catecholamines by the adrenal medulla.
Peptic Ulcer Disease
Nicotine delays healing in peptic ulcer disease; therefore, NICOTROL Inhaler therapy should be used with caution in patients with esophagitis, active gastric or peptic ulcers and only when the benefits of including nicotine replacement in a smoking cessation program outweigh the risks.
Accelerated Hypertension
Nicotine therapy constitutes a risk factor for development of malignant hypertension in patients with accelerated hypertension; therefore, NICOTROL Inhaler therapy should be used with caution in these patients and only when the benefits of including nicotine replacement in a smoking cessation program outweigh the risks.
Information for Patient
A patient information sheet is included in the package of NICOTROL Inhaler cartridges dispensed to the patient. Patients should be encouraged to read the information sheet carefully and to ask their physician and pharmacist about the proper use of the product (See DOSAGE AND ADMINISTRATION). Patients must be advised to keep both used and unused cartridges out of the reach of children and pets.
Drug Interactions
Physiological changes resulting from smoking cessation, with or without nicotine replacement, may alter the pharmacokinetics of certain concomitant medications, such as tricyclic antidepressants and theophylline. Doses of these and perhaps other medications may need to be adjusted in patients who successfully quit smoking.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Nicotine itself does not appear to be a carcinogen in laboratory animals. However, nicotine and its metabolites increased the incidences of tumors in the cheek pouches of hamsters and forestomach of F344 rats, respectively when given in combination with tumor-initiators. One study, which could not be replicated, suggested that cotinine, the primary metabolite of nicotine, may cause lymphoreticular sarcoma in the large intestine of rats. Neither nicotine nor cotinine was mutagenic in the Ames salmonella test. Nicotine-induced reparable DNA damage in an E. coli test system. Nicotine was shown to be genotoxic in a test system using Chinese hamster ovary cells. In rats and rabbits, implantation can be delayed or inhibited by a reduction in DNA synthesis that appears to be caused by nicotine. Studies have shown a decrease in litter size in rats treated with nicotine during gestation.
Pregnancy
The harmful effects of cigarette smoking on maternal and fetal health are clearly established. These include low birth weight, an increased risk of spontaneous abortion, and increased perinatal mortality. The specific effects of NICOTROL Inhaler therapy on fetal development are unknown. Therefore pregnant smokers should be encouraged to attempt cessation using educational and behavioral interventions before using pharmacological approaches.
Spontaneous abortion during nicotine replacement therapy has been reported; as with smoking, nicotine as a contributing factor cannot be excluded.
NICOTROL Inhaler therapy should be used during pregnancy only if the likelihood of smoking cessation justifies the potential risk of using it by the pregnant patient, who might continue to smoke.
Teratogenicity
Other Effects
Animal Studies
A nicotine bolus (up to 2 mg/kg) to pregnant rhesus monkeys caused acidosis, hypercarbia, and hypotension (fetal and maternal concentrations were about 20 times those achieved after smoking one cigarette in 5 minutes). Fetal breathing movements were reduced in the fetal lamb after intravenous injection of 0.25 mg/kg nicotine to the ewe (equivalent to smoking 1 cigarette every 20 seconds for 5 minutes). Uterine blood flow was reduced about 30% after infusion of 0.1 µg/kg/min nicotine to pregnant rhesus monkeys (equivalent to smoking about six cigarettes every minute for 20 minutes).
Human Experience
Cigarette smoking during pregnancy is associated with an increased risk of spontaneous abortion, low birth weight infants and perinatal mortality. Nicotine and carbon monoxide are considered the most likely mediators of these outcomes. The effects of cigarette smoking on fetal cardiovascular parameters have been studied near term. Cigarettes increased fetal aortic blood flow and heart rate and decreased uterine blood flow and fetal breathing movements. NICOTROL Inhaler therapy has not been studied in pregnant women.
Labor and Delivery
NICOTROL Inhaler is not recommended for use during labor and delivery. The effect of nicotine on a mother or the fetus during labor is unknown.
Use in Nursing Mothers
Caution should be exercised when the NICOTROL Inhaler is administered to nursing mothers. The safety of NICOTROL Inhaler therapy in nursing infants has not been examined. Nicotine passes freely into breast milk; the milk to plasma ratio averages 2.9. Nicotine is absorbed orally. An infant has the ability to clear nicotine by hepatic first-pass clearance; however, the efficiency of removal is probably lowest at birth. Nicotine concentrations in milk can be expected to be lower with NICOTROL Inhaler when used as recommended than with cigarette smoking, as maternal plasma nicotine concentrations are generally reduced with nicotine replacement. The risk of exposure of the infant to nicotine from NICOTROL Inhaler therapy should be weighed against the risks associated with the infant's exposure to nicotine from continued smoking by the mother (passive smoke exposure and contamination of breast milk with other components of tobacco smoke) and from the NICOTROL Inhaler alone, or in combination with continued smoking.
Pediatric Use
Safety and effectiveness in pediatric and adolescent patients below the age of 18 years have not been established for any nicotine replacement product. However, no specific medical risk is known or expected in nicotine dependent adolescents. NICOTROL Inhaler should be used for the treatment of tobacco dependence in the older adolescent only if the potential benefit justifies the potential risk.
Geriatric Use
Clinical studies of NICOTROL Inhaler did not include sufficient numbers of subjects age 65 and over to determine whether they respond differently from younger subjects. Other reports on clinical experience have not identified differences between older and younger patients. In general, dosage selection for an elderly patient should be cautious, usually starting at the low end of the dosage range reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease.
Adverse Reactions/Side Effects
Assessment of adverse events in the 1,439 patients (730 on active drug) who participated in controlled clinical trials (including three dose finding studies) is complicated by the occurrence of signs and symptoms of nicotine withdrawal in some patients and nicotine excess in others. The incidence of adverse events is confounded by: (1) the many minor complaints that smokers commonly have, (2) continued smoking by many patients and (3) the local irritation from both the active drug and the placebo.
Local Irritation
NICOTROL Inhaler and the placebo were both associated with local irritant side effects. Local irritation in mouth and throat was reported by 40% of patients on active drug as compared to 18% of patients on placebo. Irritant effects were higher in the two pivotal trials with higher doses being 66% on active drug and 42% on placebo. Coughing (32% active versus 12% placebo) and rhinitis (23% active versus 16% placebo) were also higher on active drug. The majority of patients rated these symptoms as mild. The frequency of cough, and mouth and throat irritation declined with continued use of NICOTROL Inhaler. Other adverse events that occurred in over 3% of patients on active drug in placebo-controlled pivotal trials considered possibly related to the local irritant effects of the NICOTROL Inhaler are taste comments, pain in jaw and neck, tooth disorders and sinusitis.
Withdrawal
Symptoms of withdrawal were common in both active and placebo groups. Common withdrawal symptoms seen in over 3% of patients on active drug included: dizziness, anxiety, sleep disorder, depression, withdrawal syndrome, drug dependence, fatigue and myalgia.
Nicotine-Related Adverse Events
The most common nicotine-related adverse event was dyspepsia. This was present in 18% of patients in the active group compared to 9% of patients in the placebo group. Other nicotine related events present in greater than 3% of patients on active drug include nausea, diarrhea, and hiccup.
Smoking Related Adverse Events
Smoking related adverse events present in greater than 3% of patients on active drug include chest discomfort, bronchitis, and hypertension.
Other Adverse Events
Adverse events of unknown relationship to nicotine occurring in greater than 3% of patients on active drug include headache (26% of patients on active and 15% of patients on placebo), influenza-like symptoms, pain, back-pain, allergy), paresthesia, flatulence and fever.
Adverse reactions not listed above that have been identified during post-marketing experience with the nicotine inhaler are listed below:
Gastrointestinal disorders: dysphagia
General disorders and administration site conditions: chest pain
Immune system disorders: anaphylactic reaction
Nervous system disorders: seizure
Skin and subcutaneous tissue disorders: rash
Related/similar drugs
Drug Abuse and Dependence
NICOTROL Inhaler is likely to have a low abuse potential based on differences between the product and cigarettes in three characteristics commonly considered important in contributing to abuse: slower absorption, smaller fluctuations in blood levels and lower blood levels of nicotine. NICOTROL Inhaler, like many other nicotine-based smoking cessation therapies, does not produce arterial concentrations similar to cigarettes. However, nicotine withdrawal symptoms were noted in clinical trials at the time of NICOTROL Inhaler tapering and after NICOTROL Inhaler discontinuation.
Dependence might occur from transference of tobacco-related nicotine dependence to the NICOTROL Inhaler. The use of the inhaler beyond 6 months has not been evaluated in clinical trials and is not recommended. To minimize the risk of dependence, patients should be encouraged to withdraw gradually from NICOTROL Inhaler therapy after 3 months of usage (See DOSAGE AND ADMINISTRATION). If necessary, dose reduction can be achieved by gradual reduction of the dose over a 6 to 12 week period.
Overdosage
Signs and Symptoms of Nicotine Toxicity
Signs and symptoms of an overdose of the NICOTROL Inhaler would be expected to be the same as those of acute nicotine poisoning including: pallor, cold sweat, nausea, salivation, vomiting, abdominal pain, diarrhea, headache, dizziness, disturbed hearing and vision, tremor, mental confusion, and weakness. Prostration, hypotension, arrhythmia, and respiratory failure may ensue with large overdoses. Lethal doses produce convulsions quickly and death follows as a result of peripheral or central respiratory paralysis or, less frequently, cardiac failure.
Overdose from Inhalation
The oral LD50 for nicotine is >5 mg/kg in dogs and >24 mg/kg in rodents. Death is due to respiratory paralysis. The oral minimum acute lethal dose for nicotine in adult humans is reported to be 40 to 60 mg (<1 mg/kg). The effects of using several cartridges in rapid succession are unknown.
Doses of nicotine that are tolerated by adult smokers during treatment may produce severe signs and symptoms of poisoning in children and may prove fatal. Suspected nicotine poisoning in a child should be considered a medical emergency and treated immediately (See WARNINGS, Safety Note Concerning Children).
One cartridge of NICOTROL Inhaler contains 10 mg nicotine, of which, approximately 4 mg is delivered nicotine. It is unlikely that an excessive nicotine overdose will occur via inhalation. Should such an overdose occur, however, with signs of nicotine poisoning, the patient should be instructed to contact his/her physician immediately. For additional emergency information, call your regional poison center or call the National Capital Poison Center toll free (1-800-222-1222).
Overdose from Ingestion
Persons ingesting NICOTROL Inhaler cartridges should be referred to a health care facility for management. In unconscious patients with a secure airway, instill activated charcoal via a nasogastric tube. A saline cathartic or sorbitol may be added to the first dose of activated charcoal. Repeated doses of activated charcoal should be administered as long as the cartridge remains in the gastrointestinal tract since it will continue to release nicotine for many hours. The NICOTROL Inhaler cartridges can be identified with a radiogram.
Management of Nicotine Poisoning
Administration of nicotine must be stopped immediately and the patient should be treated symptomatically. Other supportive measures include diazepam or barbiturates for seizures, atropine for excessive bronchial secretions or diarrhea, respiratory support for respiratory failure, and vigorous fluid support for hypotension and cardiovascular collapse.
Nicotrol Inhalant Dosage and Administration
Patients must desire to stop smoking and should be instructed to stop smoking completely as they begin using NICOTROL Inhaler. It is important that patients understand the instructions, and have their questions answered. They should clearly understand the directions for using the NICOTROL Inhaler and safely disposing of the used cartridges.
The initial dosage of NICOTROL Inhaler is individualized. Patients may self titrate to the level of nicotine they require. Most successful patients in the clinical trials used between 6 and 16 cartridges a day. Best effect was achieved by frequent continuous puffing (20 minutes). The recommended duration of treatment is 3 months, after which patients may be weaned from the NICOTROL Inhaler by gradual reduction of the daily dose over the following 6 to 12 weeks. The safety and efficacy of the continued use of NICOTROL Inhaler for periods longer than 6 months have not been studied and such use is not recommended.
Dosing recommendations are summarized in the table below.
RECOMMENDED DOSING
| Duration | Recommended Cartridges/day | |
|---|---|---|
|
INITIAL TREATMENT |
Up to 12 Weeks |
6 – 16 |
|
Gradual Reduction (if needed) |
6–12 Weeks |
No tapering strategy has been shown to be superior to any other in clinical studies. |
Initial Treatment (Up to 12 Weeks)
For best results, patients should be encouraged to use at least 6 cartridges per day at least for the first 3 to 6 weeks of treatment. In clinical trials, the average daily dose was >6 (range 3 to 18) cartridges for patients who successfully quit smoking. Additional doses may be needed to control the urge to smoke with a maximum of 16 cartridges daily for up to 12 weeks. Regular use of NICOTROL Inhaler during the first week of treatment may help patients adapt to the irritant effects of the product. Some patients may exhibit signs or symptoms of nicotine withdrawal or excess which will require an adjustment of the dosage (See Individualization of Dosage).
Gradual Reduction of Dose (Up to 12 Weeks)
Most patients will need to gradually discontinue the use of NICOTROL Inhaler after the initial treatment period. Gradual reduction of dose may begin after twelve weeks of initial treatment and may last for up to twelve weeks. Recommended strategies for discontinuing use include suggesting to patients that they use the product less frequently, keep a tally of daily usage, try to meet a steadily reducing target or set a planned quit date for stopping use of the product.
Individualization of Dosage
The NICOTROL Inhaler provides the smoker with adequate amounts of nicotine to reduce the urge to smoke, and may provide some degree of comfort by providing a hand-to-mouth ritual similar to smoking, although the importance of such an effect in smoking cessation is, as yet, unknown.
The success or failure of smoking cessation is influenced by the quality, intensity and frequency of supportive care. Patients are more likely to quit smoking if they are seen frequently and participate in formal smoking cessation programs.
The goal of NICOTROL Inhaler therapy is complete abstinence. If a patient is unable to stop smoking by the fourth week of therapy, treatment should probably be discontinued.
Patients who fail to quit on any attempt may benefit from interventions to improve their chances for success on subsequent attempts. Patients who were unsuccessful should be counseled and should then probably be given a therapeutic holiday before the next attempt. A new quit attempt should be encouraged when conditions are more favorable.
Based on the clinical trials, a reasonable approach to assisting patients in their attempt to quit smoking is to begin initial treatment, using the recommended dosage (See DOSAGE AND ADMINISTRATION). Dosage can then be adjusted in those patients with signs or symptoms of nicotine withdrawal or excess. Patients who are successfully abstinent on NICOTROL Inhaler should be treated at the selected dosage for up to 12 weeks, after which use of the Inhaler should be gradually reduced over the next 6 to 12 weeks. Some patients may not require gradual reduction of dosage and may abruptly stop treatment successfully. The safe use of this product for longer than 6 months has not been established.
The symptoms of nicotine withdrawal overlap those of nicotine excess (See CLINICAL PHARMACOLOGY Pharmacodynamics, and ADVERSE REACTIONS). Since patients using NICOTROL Inhaler may also smoke intermittently, it is sometimes difficult to determine if they are experiencing nicotine withdrawal or nicotine excess. Controlled clinical trials of nicotine products suggest that palpitations, nausea and sweating are more often symptoms of nicotine excess, whereas anxiety, nervousness and irritability are more often symptoms of nicotine withdrawal.
Storage and Handling
Disposal
See patient information sheet for instructions on handling and disposal. After using the NICOTROL Inhaler, carefully separate the mouthpiece, remove the used cartridge and throw it away, out of the reach of children and pets. Store the mouthpiece in the plastic storage case for further use. The mouthpiece is reusable and should be cleaned regularly with soap and water. The NICOTROL Inhaler cartridges can be detected on a radiogram.
How Supplied
NICOTROL INHALER (nicotine inhalation system) is supplied as 168 cartridges each containing 10 mg (4 mg is delivered) nicotine (NDC 0009-5400-01). Each unit consists of 5 mouthpieces, 28 storage trays each containing 6 cartridges and 1 plastic storage case. A patient information leaflet is enclosed with the package.
Store at room temperature not to exceed 77°F (25°C).
Protect cartridges from light.

Nicotrol® Inhaler
(nicotine inhalation system)
10 mg per cartridge
(4 mg delivered)
An Aid to Help You
Stop Smoking
Patient Information
Read and follow carefully.
If you have questions or want more information, ask your doctor or pharmacist.
IMPORTANT INFORMATION - Read carefully
- 1.
- NICOTROL Inhaler helps you quit smoking by reducing your urge to smoke. Success in quitting with nicotine replacement therapy (such as NICOTROL Inhaler) usually involves behavior change.
- •
- Your doctor may adjust the number of Inhaler cartridges during the first few weeks. As your body adjusts to not smoking, your doctor will either tell you to stop using the Inhaler or slowly reduce the dose.
- •
- People who use Nicotrol Inhaler with a comprehensive behavioral smoking cessation program are more successful in quitting smoking. This program can include support groups, counseling or specific behavior change techniques.
- 2.
- Side Effects: Many people experience mild irritation of the mouth or throat and cough when they first use the Nicotrol Inhaler. Most people get used to these effects in a short time. Stomach upset may also occur.
- 3.
- Because you are already addicted to the nicotine in cigarettes, it is possible to stay dependent on the lower dose of nicotine found in the Nicotrol Inhaler. It is important to use the Inhaler for only as long as directed by your doctor to overcome your nicotine addiction and smoking habit.
NICOTROL Inhaler Contents
WARNINGS: Read before using NICOTROL Inhaler
- 1.
-
Commit yourself - NO SMOKING! For the NICOTROL Inhaler to help, you must be firmly committed to quitting! Stop smoking as soon as you start using the Inhaler. Do not smoke or use any other tobacco products at any time while using the NICOTROL Inhaler.
- •
- Nicotine overdose can occur. If symptoms of overdose occur, call a doctor or Poison Control Center immediately. Overdose symptoms include: bad headaches, dizziness, upset stomach, drooling, vomiting, diarrhea, cold sweat, weak and irregular pulse, blurred vision, hearing difficulties, mental confusion, weakness and fainting.

- 2.
- Keep out of reach of children and pets. The NICOTROL Inhaler can cause serious illness in children and pets - even in very small amounts. If a child chews on or swallows NICOTROL Inhaler cartridges, call a doctor or Poison Control Center. After a cartridge is used, throw away out of reach of children and pets. Even used cartridges contain enough nicotine to seriously harm children and pets. The NICOTROL Inhaler is a child resistant product. Please read carefully the instructions regarding how to open, close and lock.

- 3.
- Tell your doctor if you have:
|
|
|
|

- 4.
- If you are pregnant or breast-feeding, only use this medicine on the advice of your health care provider. Smoking can seriously harm your child. Try to stop smoking without using any nicotine replacement medicine. This medicine is believed to be safer than smoking. However, the risks to your child from this medicine are not fully known.

BEFORE YOU USE - Read information on both sides. FOLLOW ALL DIRECTIONS Exactly!
- 1.

- •
- Follow doctor's directions.
- •
- Stop smoking completely during the NICOTROL Inhaler treatment program.
- 2.
- •
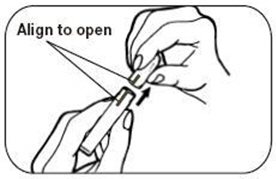
- Remove mouthpiece from plastic wrap.
- •
- Push the top and bottom together and turn the two pieces to line up the markings.
- •
- Pull the top and bottom apart.
- 3.
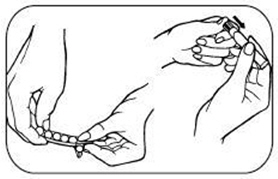
- •
- Take out cartridge tray.
- •
- Peel back to release 1 cartridge.
- •
- Insert cartridge into Inhaler.
- •
- Push hard on the cartridge until it pops down into place.
- 4.
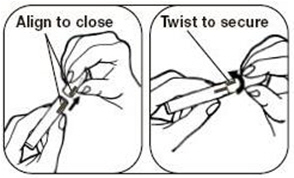
- •
- Line up the markings again and push the two pieces back together so they fit tight.
- •
- Turn the top and bottom pieces so the markings do not line up and it is locked again.
- •
- Store cartridges in plastic case when not in use.
- 5.

- •
- Inhale deeply into back of throat or puff in short breaths.
- •
- As you inhale or puff through the mouthpiece, nicotine turns into a vapor and is absorbed into your mouth and throat.
- •
- Use Inhaler longer and more often at first to help control cigarette cravings.
- 6.

- •
- Nicotine in cartridges is used up after about 20 minutes of active puffing.
- •
- Try different schedules to help control cravings. Puffing on the Inhaler for 5 min. at a time will give you enough nicotine for 4 uses. In a few days you'll find what works best and know when nicotine in cartridges is used up.
- •
- Use Inhaler at room temperature (above 60°F), cold temperatures reduce amount of nicotine you inhale.
- 7.
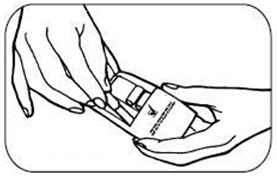
- •
- When cartridge is empty, take off top of mouthpiece.
- •
- Throw used cartridge away, out of reach of children and pets.
- •
- When not in use keep the mouthpiece in the locked position and always store mouthpiece and cartridges in plastic case, out of reach of children and pets.
- 8.
- READ & FOLLOW:
- •
- Side Effects: You may experience mild irritation of the mouth or throat and cough when you first use the Nicotrol Inhaler. You should get used to these effects in a short time. Stomach upset may also occur.
- •
- Do not use more than 16 cartridges each day unless directed to do so by your doctor.
- •
- Do not use longer than 6 months.
- •
- Store cartridges at room temperature, not to exceed 77°F (25°C).
- •
- If you keep cartridges in car, be careful: interiors heat up quickly.
- •
- Protect from light.
- •
- Clean mouthpiece regularly with soap and water.
QUESTIONS? Call 1-888-642-6876

LAB-0345-5.0
Revised July 2024
PRINCIPAL DISPLAY PANEL - 6 Cartridge Tray
Nicotrol® Inhaler
(nicotine inhalation system)
Rx only
10 mg/cartridge
(4 mg delivered)
FOR ORAL INHALATION USE ONLY
KEEP OUT OF THE REACH OF CHILDREN.
EACH CARTRIDGE IS CHILD RESISTANT.
DOSAGE: See Patient Insert for use
and disposal information.
Distributed by Pharmacia & Upjohn Co
Division of Pfizer Inc, NY, NY 10017
DO NOT USE IF SEAL ON TRAY IS BROKEN
Store at room temperature, not to exceed
77°F (25°C). Protect from light.
6 Cartridges
820 677 000
© 2007 Pharmacia & Upjohn Company LLC
MADE IN SWEDEN
870154
| NICOTROL
nicotine inhalant |
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
| Labeler - Pharmacia & Upjohn Company LLC (618054084) |
Frequently asked questions
- How long does nicotine withdrawal last?
- How long does nicotine stay in your system? Detection times and testing
- What are the side effects of vaping?
More about Nicotrol Inhaler (nicotine)
- Check interactions
- Compare alternatives
- Reviews (40)
- Latest FDA alerts (1)
- Side effects
- Dosage information
- During pregnancy
- Drug class: smoking cessation agents
- Breastfeeding
- En español
Patient resources
Professional resources
Other brands
Nicoderm CQ, Nicorette, Nicotrol NS