Diabetic nephropathy
Medically reviewed by Drugs.com. Last updated on Jan 10, 2025.
What is Diabetic nephropathy?
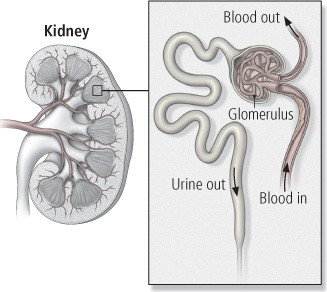
Diabetic nephropathy is kidney disease that is a complication of diabetes. It can occur in people with type 2 diabetes, the diabetes type that is most common and is caused by resistance to insulin, or in people with type 1 diabetes, the type that more often begins at an early age and results from decreased insulin production. Diabetic nephropathy is caused by damage to the tiniest blood vessels. When small blood vessels begin to develop damage, both kidneys begin to leak proteins into the urine. As damage to the blood vessels continues, the kidneys gradually lose their ability to remove waste products from the blood.
|
|
Up to 40% of people with type 1 diabetes eventually develop significant kidney disease, which sometimes requires dialysis or a kidney transplant. Only 4% to 6% of all type 2 diabetes patients end up requiring dialysis, although about 20% to 30% of people with type 2 diabetes will develop at least some kidney damage. About 40% of all people who need to start dialysis have kidney failure from type 1 or type 2 diabetes.
Symptoms
There are usually no symptoms in the early stages of diabetic nephropathy. When symptoms do begin to appear, they may include ankle swelling and mild fatigue. Later symptoms include extreme fatigue, nausea, vomiting, and urinating less than usual.
Diagnosis
The first sign of kidney damage is protein in the urine, which a doctor can measure in microscopic amounts, called microalbuminuria. Small amounts of albumin show up in the urine five to 10 years before major kidney damage happens.
If you have diabetes, your doctor will suggest regular monitoring of urine, and blood tests to check the health of your kidneys.
Occasionally, a doctor may be concerned that kidney injury in a diabetic person is related to a separate problem. In that case, other tests such as ultrasound or a kidney biopsy may be recommended. In a biopsy, a small piece of kidney tissue is removed through a needle and examined in a laboratory.
Expected duration
Kidney disease can't be reversed once damage is done. Kidney disease from diabetes is progressive, meaning it continues to get worse. However, good control of blood sugar and blood pressure and treatment with medicine from either of two drug groups (see prevention, below) can slow the progression of the disease.
Prevention
The best way to prevent diabetic nephropathy is to control your blood sugar and to keep your blood pressure in the normal range. The systolic pressure, the "top" blood pressure number, should be consistently lower than 130 millimeters of mercury (mm Hg).
Two types of blood pressure medicines protect against kidney damage in ways that go beyond lowering your blood pressure. Any person who has diabetes and who also has high blood pressure should regularly take one of these medications. These medicines come from a group of drugs called angiotensin-converting–enzyme inhibitors (ACE inhibitors), including lisinopril (Zestril, Prinivil), enalapril (Vasotec), moexipril (Univasc), benazepril (Lotensin), and others, or from a group of drugs called angiotensin-receptor blockers (ARBs), including losartan (Cozaar), valsartan (Diovan), and others.
Avoiding medications that can sometimes have harmful side effects upon the kidneys also can help to prevent kidney disease. If you have severe kidney disease, your doctor may advise you to avoid pain medications in the nonsteroidal anti-inflammatory drug group (NSAID group) such as ibuprofen.
A low-protein diet (10% to 12% or less of total calories) also may slow or halt the progression of kidney disease. If you smoke cigarettes, you should quit.
Drugs used to treat this and similar conditions
Treatment
If you have diabetes with microalbuminuria or blood test evidence of kidney disease, you can slow the progression of kidney disease by taking a drug called an SGLT2 inhibitor. Examples of SGLT2 inhibitors approved to help preserve kidney function even in people without diabetes include canagliflozin (Invokana) and dapagliflozin (Farxiga). If you have diabetes and high blood pressure, doctors usually prescribe a medication from the ACE inhibitor or ARB group as part of the hypertension treatment program. These medications slow the progression of kidney disease in people with diabetes, although kidney disease continues to develop gradually. These two medicine groups are closely related, so the drugs usually are not combined with each other.
Reducing the amount of protein in your diet also may be helpful to slow progressing kidney disease.
Once nephropathy reaches advanced stages, you may need dialysis to remove waste products from the blood. There are two types of dialysis, hemodialysis and peritoneal dialysis.
Hemodialysis filters waste substances and excess fluid out of the blood. Hemodialysis usually is done at a dialysis center in three- to four-hour sessions three times a week. Peritoneal dialysis does not directly filter the blood. Instead, for this form of dialysis, sterile fluid is allowed to flow into the abdominal cavity through a catheter that is permanently placed through the skin. The fluid is then removed after it has absorbed waste substances.
After practice, peritoneal dialysis can be done at home. It is a good alternative for some people, although it requires significant time and self-care.
An alternative way to treat advanced kidney disease is with a kidney transplant. Kidney transplants have allowed many people with severe kidney disease to avoid or discontinue dialysis. However, the donor and the recipient have to match genetically, or the body will reject the new kidney. The waiting period for a matching donated kidney is between two and six years.
Anti-rejection drugs that suppress the immune system help the body to accept the donated organ. An organ recipient can expect to take such medications as long as the transplanted kidney continues to function. A transplanted kidney is likely to function for at least 10 years if its genetics are closely matched. If a transplanted kidney stops functioning, dialysis or a new transplant is necessary.
In a person with type 1 diabetes and kidney failure, a kidney-pancreas transplant is another possible treatment. This option is available only for a small number of people because of the scarcity of organ donors, the risks of the surgery, and the need for lifelong immunosuppressive drugs. When it is successful, the transplanted pancreas begins producing insulin and may reverse diabetes.
Treatment options
The following list of medications are related to or used in the treatment of this condition.
When to call a professional
If you have diabetes, your blood pressure should be checked every six months to a year, or more often if it is higher than goal. If you have not been diagnosed with diabetic nephropathy, your urine should be tested for microalbumin at least once a year to check for this problem and diagnose it as early as possible. People with kidney disease need to have regular tests of kidney function — once a year or more often. If you have symptoms that suggest advanced kidney disease, you should discuss them with your physician.
Prognosis
Although kidney failure cannot always be prevented, worsening can be slowed with medications and control of risk factors. When full kidney failure occurs, dialysis and a kidney transplant are options that allow people to continue to lead active lives.
Additional info
National Institute of Diabetes and Digestive and Kidney Disorders
https://www.niddk.nih.gov/
American Diabetes Association
https://www.diabetes.org/
Learn more about Diabetic nephropathy
Treatment options
Care guides
Further information
Always consult your healthcare provider to ensure the information displayed on this page applies to your personal circumstances.