Above the Knee Amputation
Medically reviewed by Drugs.com. Last updated on Aug 4, 2025.
What do I need to know about an above the knee amputation?
Above the knee amputation is surgery to remove your leg above your knee cap. You may need an amputation because of an injury, a tumor, or an infection. Problems with your leg veins or arteries, or complications of diabetes may also cause you to need an amputation. The part of your leg that is not removed is called a residual limb. You will be shown how to care for your residual limb. You can also work with specialists to have prosthetics made for you. A prosthetic will help you return to your normal daily activities.
How do I prepare for an above the knee amputation?
- If you are having scheduled surgery, your healthcare provider will talk to you about how to prepare. He or she may tell you not to eat or drink anything after midnight on the day of your surgery. He or she will tell you what medicines to take or not take on the day of your surgery. You may be given an antibiotic through your IV to help prevent a bacterial infection. Tell your healthcare provider if you have ever had an allergic reaction to an antibiotic.
- An angiogram may be needed to check the blood flow in your leg. A catheter (thin tube) is threaded into an artery in your groin. Contrast liquid is put into the catheter. X-rays are then taken to watch how the liquid and blood flow through your leg. Tell your healthcare provider if you have ever had an allergic reaction to contrast liquid. Another test may be done to test the oxygen levels in your leg. These tests help healthcare providers decide where your leg needs to be amputated.
Related medications
What happens during an above the knee amputation?
- You will be given general anesthesia to keep you asleep and free from pain during surgery. An incision will be made in your leg above your knee. The part of your leg below that will be removed, and your thigh bone will be made smooth. A flap made of muscle, tissue, and skin may be used to cover the end of your bone. Tissue for the flap may come from other parts of your leg or foot.
- If your leg was infected before surgery, healthcare providers may not put stitches or staples in to close it right away. The incision may be left open for several days after surgery. If you did not have an infection, the flap will be closed with stitches. The stitches may be taken out about a month after surgery. Your healthcare provider may place a drain near your wound. The drain can help remove blood or extra fluid from your incision. This will help your limb heal faster.
- A soft or hard bandage will be put over your residual limb. A soft bandage will be used if the incision was left open. The bandage will be covered with an elastic wrap. A cast will be put over the bandage if the incision was closed with stitches. The cast protects your residual limb from injury. The cast also makes fitting for a prosthesis easier and quicker. A prosthesis may be put on right after surgery.
What happens after an above the knee amputation?
You may continue to feel the part of your leg that has been amputated. These are called phantom feelings. These feelings are normal and may or may not be painful.
- Drains are thin rubber tubes put into your skin to drain fluid from around your incision. The drains are taken out when the incision stops draining.
- Take deep breaths and cough 10 times each hour. This will decrease your risk for a lung infection. Take a deep breath and hold it for as long as you can. Let the air out and then cough strongly. Deep breaths help open your airway. You may be given an incentive spirometer to help you take deep breaths. Put the plastic piece in your mouth and take a slow, deep breath, then let the air out and cough. Repeat these steps 10 times every hour.
- Activity guidelines:
- Change your position often while you are resting in bed. This moves fluids in your lungs, helping decrease your risk for pneumonia. This also helps prevent skin pressure sores, and keeps your muscles and tendons from tightening.
- While you are in bed, keep your residual limb raised on one to two pillows for the first 24 hours after surgery. This helps decrease swelling.
- After the first day, keep your residual limb flat on the bed to prevent your hip from tightening.
- Lie on your stomach twice a day. This also helps prevent hip tightening.
- Start exercising your other leg and residual limb as soon as healthcare providers say it is okay. Lift your leg off the bed and move it in big circles. This helps strengthen your leg, and may prevent blood clots from forming. Repeat with your residual limb.
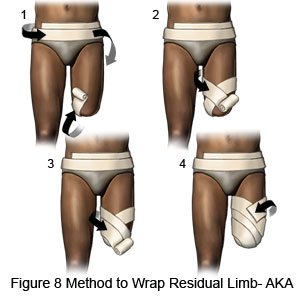
- Wrap your residual limb. Healthcare providers will teach you or a family member how to wrap your residual limb with an elastic bandage. This helps to control swelling, and helps to form the residual limb into a firm cone shape. This shape will fit into a prosthesis. Healthcare providers may start wrapping your residual limb within 1 to 3 days after surgery, or they may wait until the cast is removed. At first, healthcare providers will not pull the elastic bandage very tight. They will pull the bandage tighter as your wound heals and the stitches are removed. They will rewrap your residual limb about every 4 hours to keep the bandage smooth and tight. Ask your healthcare provider to rewrap the bandage if your pain is worse. This may mean the bandage is too tight.
What are the risks of an above the knee amputation?
During or after surgery, you may bleed more than expected. Blood may collect under your skin and form a lump called a hematoma. This may need to be drained to prevent infection. It may be difficult for your wound to heal and you may get a wound infection. You may get a blood clot in your leg or arm. This can cause pain and swelling, and it can stop blood from flowing where it needs to go in your body. The blood clot can break loose and travel to your lungs or brain. A blood clot in your lungs can cause chest pain and trouble breathing. A blood clot in your brain can cause a stroke. These problems can be life-threatening.
Care Agreement
You have the right to help plan your care. Learn about your health condition and how it may be treated. Discuss treatment options with your healthcare providers to decide what care you want to receive. You always have the right to refuse treatment. The above information is an educational aid only. It is not intended as medical advice for individual conditions or treatments. Talk to your doctor, nurse or pharmacist before following any medical regimen to see if it is safe and effective for you.© Copyright Merative 2025 Information is for End User's use only and may not be sold, redistributed or otherwise used for commercial purposes.
Further information
Always consult your healthcare provider to ensure the information displayed on this page applies to your personal circumstances.