Laparoscopic Cholecystectomy
Medically reviewed by Drugs.com. Last updated on May 6, 2024.
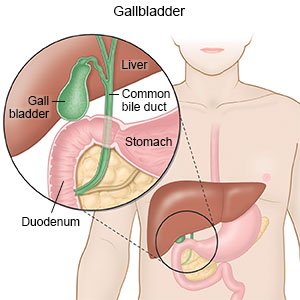
What do I need to know about a laparoscopic cholecystectomy?
Laparoscopic cholecystectomy is surgery to remove gallstones and your gallbladder.
 |
How do I prepare for surgery?
- Your surgeon will tell you how to prepare. You may be told not to eat or drink anything after midnight on the day of surgery. Arrange to have someone drive you home after surgery and stay with you for 24 hours.
- Tell your surgeon all the medicines you currently take. He or she will tell you if you need to stop any medicine for surgery, and when to stop. He or she will tell you which medicines to take or not take on the day of surgery.
- You may need blood or urine tests. You may also need x-rays, an ultrasound, or a CT scan. Tell your surgeon if you had an allergic reaction to contrast liquid. Tell your surgeon about any allergies you have, including medicines and anesthesia.
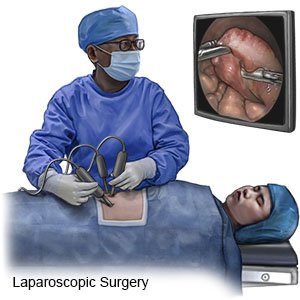
What will happen during surgery?
- Your surgeon will make between 1 and 4 small incisions in your abdomen or belly button. He or she will insert small tools into the incisions. Your abdomen will be filled with carbon dioxide gas to make it swell. This helps your surgeon see your organs better and gives more room to move the tools around.
- Your surgeon will look for and remove gallstones in and around your gallbladder. X-rays or an ultrasound may be used. Your surgeon will remove your gallbladder through one of the incisions. The carbon dioxide will be released from your abdomen. The incisions will be closed with stitches, medical glue, or adhesive strips, then covered with bandages.
What should I expect after surgery?
You will be taken to a recovery room until you are fully awake. Healthcare providers will monitor you closely for any problems. Providers will help you walk around to prevent blood clots. You may be able to go home later the same day, or you may stay in the hospital overnight.
- Pain, a sore throat, nausea, and vomiting are common after this surgery. These should get better within a few days. You may also have diarrhea that lasts up to a few months.
- Medicines may be given to prevent or treat pain, nausea, and vomiting. Medicines may also be given to prevent a bacterial infection. Blood thinners may be given to prevent blood clots. You may bleed or bruise more easily while you are taking blood thinners.
- Your surgeon will tell you when to remove the bandages covering the surgery area. He or she will tell you when it is okay to start bathing. You may need to take showers instead of baths for a few days.
- Your surgeon will tell you when you can drive, return to work, and do your regular daily activities.
- You will be shown how to care for the surgery area and check for signs of infection. You will also be told which foods to eat in the days and weeks after surgery.
What are the risks of a laparoscopic cholecystectomy?
- You could bleed more than expected or get an infection. Any carbon dioxide gas still in your body can cause neck and shoulder pain. Your gallbladder may leak bile into your abdomen during or after surgery. This can cause a severe infection or an abscess.
- You may still have gallstones after surgery. You may need a different procedure to remove them. Your surgeon may need to make a larger incision than expected during surgery. Your bile duct, bowel, or other organs could be damaged during surgery. This can be life-threatening.
Care Agreement
You have the right to help plan your care. Learn about your health condition and how it may be treated. Discuss treatment options with your healthcare providers to decide what care you want to receive. You always have the right to refuse treatment. The above information is an educational aid only. It is not intended as medical advice for individual conditions or treatments. Talk to your doctor, nurse or pharmacist before following any medical regimen to see if it is safe and effective for you.© Copyright Merative 2024 Information is for End User's use only and may not be sold, redistributed or otherwise used for commercial purposes.
Further information
Always consult your healthcare provider to ensure the information displayed on this page applies to your personal circumstances.