Sorine Dosage
Generic name: Sotalol Hydrochloride 80mg
Dosage form: tablet
Drug classes: Group III antiarrhythmics, Non-cardioselective beta blockers
Medically reviewed by Drugs.com. Last updated on Jan 16, 2024.
General Safety Measures for Initiation of Oral Sotalol Therapy
Withdraw other antiarrhythmic therapy before starting SORINE (sotalol hydrochloride) tablets and monitor carefully for a minimum of 2 to 3 plasma half-lives if the patient's clinical condition permits [see Drug Interactions (7)].
Hospitalize patients initiated or re-initiated on sotalol for at least 3 days or until steady-state drug levels are achieved, in a facility that can provide cardiac resuscitation and continuous electrocardiographic monitoring. Initiate oral sotalol therapy in the presence of personnel trained in the management of serious arrhythmias. Perform a baseline ECG to determine the QT interval and measure and normalize serum potassium and magnesium levels before initiating therapy. Measure serum creatinine and calculate an estimated creatinine clearance in order to establish the appropriate dosing interval (insert cross ref to renal dosing). Continually monitor patients with each uptitration in dose, until they reach steady state. Determine QTc 2 to 4 hours after every dose.
Discharge patients on sotalol therapy from an in-patient setting with an adequate supply of sotalol to allow uninterrupted therapy until the patient can fill a sotalol prescription.
Advise patients who miss a dose to take the next dose at the usual time. Do not double the dose or shorten the dosing interval.
Adult Dose for Ventricular Arrhythmias
The recommended initial dose is 80 mg twice daily. This dose may be increased in increments of 80 mg per day every 3 days provided the QTc <500 msec [see Warnings and Precautions (5.1)]. Continually monitor patients until steady state blood levels are achieved. In most patients, a therapeutic response is obtained at a total daily dose of 160 to 320 mg/day, given in two or three divided doses (because of the long terminal elimination half-life of sotalol, dosing more than a two times a day is usually not necessary). Oral doses as high as 480 to 640 mg/day have been utilized in patients with refractory life-threatening arrhythmias.
Adult Dose for Prevention of Recurrence of AFIB/AFL
The recommended initial dose is 80 mg twice daily. This dose may be increased in increments of 80 mg per day every 3 days provided the QTc <500 msec [see Warnings and Precautions (5.1)]. Continually monitor patients until steady state blood levels are achieved. Most patients will have satisfactory response with 120 mg twice daily. Initiation of sotalol in patients with creatinine clearance <40 mL/min or QTc >450 is contraindicated [see Contraindication (4)].
Pediatric Dose for Ventricular Arrhythmias or AFIB/AFL
Use the same precautionary measures for children as you would use for adults when initiating and re-initiating sotalol treatment.
For children aged about 2 years and older
For children aged about 2 years and older, with normal renal function, doses normalized for body surface area are appropriate for both initial and incremental dosing. Since the Class III potency in children is not very different from that in adults, reaching plasma concentrations that occur within the adult dose range is an appropriate guide [see Clinical Pharmacology (12.1, 12.3)].
From pediatric pharmacokinetic data the following is recommended:
For initiation of treatment, 30 mg/m2 three times a day (90 mg/m2 total daily dose) is approximately equivalent to the initial 160 mg total daily dose for adults. Subsequent titration to a maximum of 60 mg/m2 (approximately equivalent to the 360 mg total daily dose for adults) can then occur. Titration should be guided by clinical response, heart rate and QTc, with increased dosing being preferably carried out in-hospital. At least 36 hours should be allowed between dose increments to attain steady-state plasma concentrations of sotalol in patients with age-adjusted normal renal function.
For children aged about 2 years or younger
For children aged about 2 years or younger, the above pediatric dosage should be reduced by a factor that depends heavily upon age, as shown in the following graph, age plotted on a logarithmic scale in months.
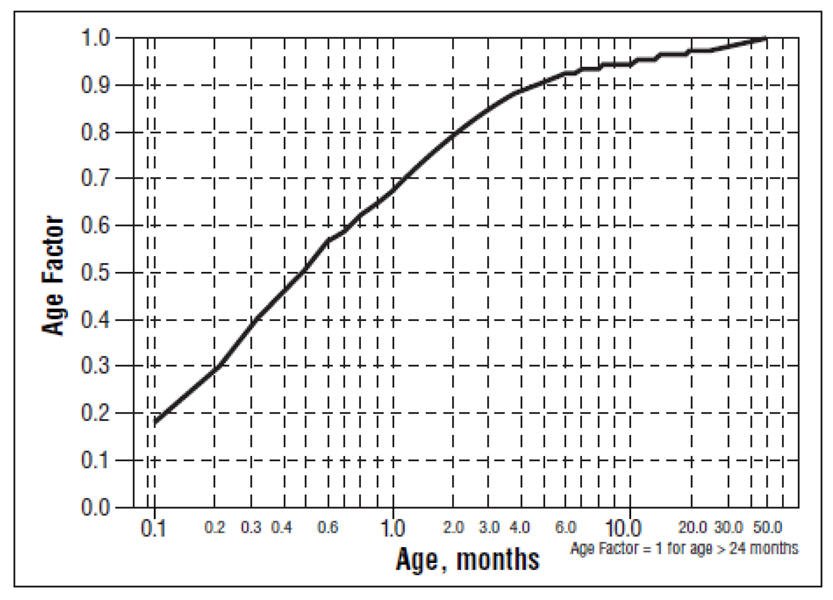
For a child aged 20 months, the dosing suggested for children with normal renal function aged 2 years or greater should be multiplied by about 0.97; the initial starting dose would be (30 × 0.97) = 29.1 mg/m2, administered three times daily. For a child aged 1 month, the starting dose should be multiplied by 0.68; the initial starting dose would be (30 × 0.68) = 20 mg/m2, administered three times daily. For a child aged about 1 week, the initial starting dose should be multiplied by 0.3; the starting dose would be (30 × 0.3) = 9 mg/m2. Use similar calculations for dose titration.
Since the half-life of sotalol decreases with decreasing age (below about 2 years), time to steady-state will also increase. Thus, in neonates the time to steady-state may be as long as a week or longer.
Dosage for Patients with Renal Impairment
Adults
Use of sotalol in any age group with decreased renal function should be at lower doses or increased intervals between doses. It will take much longer to reach steady-state with any dose and/or frequency of administration. Closely monitor heart rate and QTc.
Dose escalations in renal impairment should be done after administration of at least 5 doses at appropriate intervals (Table 1). Sotalol is partly removed by dialysis; specific advice is unavailable on dosing patients on dialysis.
The initial dose of 80 mg and subsequent doses should be administered at the intervals listed in Table 1 or Table 2.
| Creatinine Clearance mL/min | Dosing Interval (hours) |
|---|---|
| >60 | 12 |
| 30 to 59 | 24 |
| 10 to 29 | 36 to 48 |
| <10 | Dose should be individualized |
| Creatinine Clearance mL/min | Dosing Interval (hours) |
|---|---|
| >60 | 12 |
| 40 to 59 | 24 |
| <40 | Contraindicated |
Preparation of Extemporaneous Oral Solution
Sotalol hydrochloride Syrup 5 mg/mL can be compounded using Simple Syrup containing 0.1% sodium benzoate (Syrup, NF) as follows:
- Measure 120 mL of Simple Syrup.
- Transfer the syrup to a 6-ounce amber plastic (polyethylene terephthalate [PET]) prescription bottle. An oversized bottle is used to allow for a headspace, so that there will be more effective mixing during shaking of the bottle.
- Add five (5) SORINE (sotalol hydrochloride) 120 mg tablets to the bottle. These tablets are added intact; it is not necessary to crush the tablets. The addition of the tablets can also be done first. The tablets can also be crushed if preferred. If the tablets are crushed, care should be taken to transfer the entire quantity of tablet powder into the bottle containing the syrup.
- Shake the bottle to wet the entire surface of the tablets. If the tablets have been crushed, shake the bottle until the endpoint is achieved.
- Allow the tablets to hydrate for at least two hours.
- After at least two hours have elapsed, shake the bottle intermittently over the course of at least another two hours until the tablets are completely disintegrated. The tablets can be allowed to hydrate overnight to simplify the disintegration process.
The endpoint is achieved when a dispersion of fine particles in the syrup is obtained.
This compounding procedure results in a solution containing 5 mg/mL of sotalol hydrochloride. The fine solid particles are the water-insoluble inactive ingredients of the tablets.
Stability studies indicate that the suspension is stable for three months when stored at 15°C to 30°C (59°F to 86°F) [See USP Controlled Room Temperature] and ambient humidity.
Frequently asked questions
More about Sorine (sotalol)
- Check interactions
- Compare alternatives
- Pricing & coupons
- Drug images
- Side effects
- Dosage information
- During pregnancy
- Drug class: group III antiarrhythmics
- Breastfeeding
- En español
Patient resources
Other brands
Professional resources
Other brands
Related treatment guides
Further information
Always consult your healthcare provider to ensure the information displayed on this page applies to your personal circumstances.
