Maxipime Dosage
Generic name: CEFEPIME HYDROCHLORIDE 1g
Dosage form: injection, powder, for solution
Drug class: Fourth generation cephalosporins
Medically reviewed by Drugs.com. Last updated on Nov 17, 2023.
Dosage for Adults
The recommended adult dosages and routes of administration are outlined in Table 1 below for patients with creatinine clearance greater than 60 mL/min. Administer MAXIPIME intravenously over approximately 30 minutes.
| *or until resolution of neutropenia. In patients whose fever resolves but who remain neutropenic for more than 7 days, the need for continued antimicrobial therapy should be re-evaluated frequently. **Intramuscular route of administration is indicated only for mild to moderate, uncomplicated or complicated UTIs due to E. coli. §For P. aeruginosa, use 2 g IV every 8 hours. |
|||
|
Site and Type of Infection |
Dose |
Frequency |
Duration |
|
(days) |
|||
|
Adults |
Intravenous (IV)/Intramuscular (IM) |
||
|
Moderate to Severe Pneumonia§ |
1 to 2 g IV |
Every 8 to |
10 |
|
Empiric therapy for febrile neutropenic patients |
2 g IV |
Every 8 hours |
7* |
|
Mild to Moderate Uncomplicated or Complicated Urinary Tract Infections, including pyelonephritis |
0.5 to 1 g IV/IM** |
Every 12 hours |
7 to 10 |
|
Severe Uncomplicated or Complicated Urinary Tract Infections, including pyelonephritis |
2 g IV |
Every 12 hours |
10 |
|
Moderate to Severe Uncomplicated Skin and Skin Structure Infections |
2 g IV |
Every 12 hours |
10 |
|
Complicated Intra-abdominal Infections§ (used in combination with metronidazole) |
2 g IV |
Every 8 to |
7 to 10 |
Pediatric Patients (2 months up to 16 years)
The maximum dose for pediatric patients should not exceed the recommended adult dose.
The usual recommended dosage in pediatric patients up to 40 kg in weight for durations as given above for adults is:
- •
- 50 mg per kg per dose, administered every 12 hours for uncomplicated and complicated urinary tract infections (including pyelonephritis), uncomplicated skin and skin structure infections, and pneumonia (see below).
- •
- For moderate to severe pneumonia due to P. aeruginosa give 50 mg per kg per dose, every
8 hours. - •
- 50 mg per kg per dose, every 8 hours for febrile neutropenic patients.
Dosage Adjustments in Patients with Renal Impairment
Adult Patients
Adjust the dose of MAXIPIME in patients with creatinine clearance less than or equal to 60 mL/min to compensate for the slower rate of renal elimination. In these patients, the recommended initial dose of MAXIPIME should be the same as in patients with CrCL greater than 60 mL/min except in patients undergoing hemodialysis. The recommended doses of MAXIPIME in patients with renal impairment are presented in Table 2.
When only serum creatinine is available, the following formula (Cockcroft and Gault equation)1 may be used to estimate creatinine clearance. The serum creatinine should represent a steady state of renal function:
|
Males: Creatinine Clearance (mL/min) = |
Weight (kg) x (140 – age) |
|
72 × serum creatinine (mg/dL) |
|
|
Females: 0.85 × above value |
|
|
||||
|
Creatinine |
Recommended Maintenance Schedule |
|||
|
Greater than 60 |
500 mg every |
1 g every |
2 g every |
2 g every 8 hours |
|
30 to 60 |
500 mg every 24 hours |
1 g every 24 hours |
2 g every 24 hours |
2 g every 12 hours |
|
11 to 29 |
500 mg every 24 hours |
500 mg every 24 hours |
1 g every 24 hours |
2 g every 24 hours |
|
Less than 11 |
250 mg every 24 hours |
250 mg every 24 hours |
500 mg every 24 hours |
1 g every 24 hours |
|
Continuous Ambulatory Peritoneal Dialysis (CAPD) |
500 mg every 48 hours |
1 g every 48 hours |
2 g every 48 hours |
2 g every 48 hours |
|
Hemodialysis* |
1 g on day 1, then 500 mg every 24 hours thereafter |
1 g every 24 hours |
||
In patients undergoing Continuous Ambulatory Peritoneal Dialysis (CAPD), MAXIPIME may be administered at the recommended doses at a dosage interval of every 48 hours (see Table 2).
In patients undergoing hemodialysis, approximately 68% of the total amount of cefepime present in the body at the start of dialysis will be removed during a 3-hour dialysis period. The dosage of MAXIPIME for hemodialysis patients is 1 g on Day 1 followed by 500 mg every 24 hours for the treatment of all infections except febrile neutropenia, which is 1 g every 24 hours.
MAXIPIME should be administered at the same time each day and following the completion of hemodialysis on hemodialysis days (see Table 2).
Pediatric Patients
Data in pediatric patients with impaired renal function are not available; however, since cefepime pharmacokinetics are similar in adults and pediatric patients [see Clinical Pharmacology (12.3)], changes in the dosing regimen proportional to those in adults (see Tables 1 and 2) are recommended for pediatric patients.
Preparation of MAXIPIME for Intravenous Infusion
Vials
- •
- Constitute the 0.5 gram, 1 gram, or 2 grams vial, of MAXIPIME with the one of the following diluents:
- o
- Sterile Water for Injection
- o
- 0.9% Sodium Chloride Injection
- o
- 5% Dextrose Injection
- o
- 0.5% or 1% Lidocaine Hydrochloride Injection
- o
- Sterile Bacteriostatic Water for Injection with Parabens or Benzyl Alcohol
- •
- Dilute the reconstituted solution with one of the following compatible infusion solutions prior to intravenous infusion (Refer to Table 3 below for the amount of diluent to be added to each vial and the amount of the reconstituted solution to be withdrawn):
- o
- 0.9% Sodium Chloride Injection
- o
- 5% and 10% Dextrose Injection
- o
- M/6 Sodium Lactate Injection
- o
- 5% Dextrose and 0.9% sodium Chloride Injection
- o
- Lactated Rings and 5% Dextrose Injection
- o
- Normosol™-R and Normosol™-M in 5% Dextrose Injection
- •
- Parenteral drugs should be inspected visually for particulate matter before administration. If particulate matter is evident in reconstituted fluids, the drug solution should be discarded.
- •
- Administer the resulting intravenous infusion over approximately 30 minutes.
- •
- Intermittent intravenous infusion with a Y-type administration set can be accomplished with compatible solutions. However, during infusion of a solution containing cefepime, it is desirable to discontinue the other solution.
ADD-Vantage Vials
Constitute only with 50 mL or 100 mL of 5% Dextrose Injection or 0.9% Sodium Chloride Injection in ADD-Vantage flexible diluent containers as described in the instructions for reconstitution [see Dosage and Administration (2.7)].
Preparation for Intramuscular Administration
Constitute MAXIPIME vials 0.5 gram, 1 gram and 2 grams with one of the following diluents: Sterile Water for Injection, 0.9% Sodium Chloride, 5% Dextrose Injection, 0.5% or 1% Lidocaine Hydrochloride, or Sterile Bacteriostatic Water for Injection with Parabens or Benzyl Alcohol. Refer to Table 3 below for the amount of diluent to be added to each vial and the amount of reconstituted volume to be withdrawn.
Parenteral drugs should be inspected visually for particulate matter before administration. If particulate matter is evident in reconstituted fluids, the drug solution should be discarded.
| Single-Dose Vials for Intravenous (IV)/Intramuscular (IM)Administration | Amount of Diluent to be added (mL) | Approximate Cefepime Concentration (mg/mL) | Amount of Reconstituted Volume to be Withdrawn (mL) |
| Cefepime vial content | |||
| 500 mg (IV) | 5 | 100 | 5 |
| 500 mg (IM) | 1.3 | 280 | 1.8 |
| 1 g (IV) | 10 | 100 | 10.5 |
| 1 g (IM) | 2.4 | 280 | 3.6 |
| 2 g (IV) | 10 | 160 | 12.5 |
| ADD-Vantage Vials for Intravenous (IV) Administration | Amount of Diluent to be added (mL) | Approximate Cefepime Concentration (mg/mL) | Approximate Available Volume for Withdrawal (mL) |
| ADD-Vantage | |||
| 1 g vial | 50 | 20 | 50 |
| 1 g vial | 100 | 10 | 100 |
| 2 g vial | 50 | 40 | 50 |
| 2 g vial | 100 | 20 | 100 |
Compatibility and Stability
Intravenous MAXIPIME
Intravenous Infusion Compatibility
MAXIPIME vials are compatible at concentrations between 1 mg per mL and 40 mg per mL with the following intravenous infusion fluids: 0.9% Sodium Chloride Injection, 5% and 10% Dextrose Injection, M/6 Sodium Lactate Injection, 5% Dextrose and 0.9% Sodium Chloride Injection, Lactated Ringers and 5% Dextrose Injection, Normosol™-R, and Normosol™-M in 5% Dextrose Injection. These solutions may be stored up to 24 hours at controlled room temperature 20°C to 25°C (68°F to 77°F) or 7 days in a refrigerator 2°C to 8°C (36°F to 46°F).
MAXIPIME in ADD-Vantage vials are stable at concentrations of 10 to 40 mg per mL in 5% Dextrose Injection or 0.9% Sodium Chloride Injection for 24 hours at controlled room temperature 20°C to 25°C (68°F to 77°F) or 7 days in a refrigerator 2°C to 8°C (36°F to 46°F).
Admixture Compatibility
MAXIPIME admixture compatibility information is summarized in Table 4.
| NS = 0.9% Sodium Chloride Injection. D5W = 5% Dextrose Injection. na = not applicable. RT/L = Ambient room temperature and light. |
||||
|
Stability Time for |
||||
|
MAXIPIME |
Admixture and |
Intravenous (IV) Infusion Solutions |
RT/L |
Refrigeration |
|
40 mg/mL |
Amikacin 6 mg/mL |
NS or D5W |
24 hours |
7 days |
|
40 mg/mL |
Ampicillin 1 mg/mL |
D5W |
8 hours |
8 hours |
|
40 mg/mL |
Ampicillin 10 mg/mL |
D5W |
2 hours |
8 hours |
|
40 mg/mL |
Ampicillin 1 mg/mL |
NS |
24 hours |
48 hours |
|
40 mg/mL |
Ampicillin 10 mg/mL |
NS |
8 hours |
48 hours |
|
4 mg/mL |
Ampicillin 40 mg/mL |
NS |
8 hours |
8 hours |
|
4 to 40 mg/mL |
Clindamycin Phosphate 0.25 to 6 mg/mL |
NS or D5W |
24 hours |
7 days |
|
4 mg/mL |
Heparin 10 to 50 units/mL |
NS or D5W |
24 hours |
7 days |
|
4 mg/mL |
Potassium Chloride 10 to 40 mEq/L |
NS or D5W |
24 hours |
7 days |
|
4 mg/mL |
Theophylline 0.8 mg/mL |
D5W |
24 hours |
7 days |
|
1 to 4 mg/mL |
na |
Aminosyn™ II 4.25% with electrolytes and calcium |
8 hours |
3 days |
|
0.125 to 0.25 mg/mL |
na |
Inpersol™ with 4.25% dextrose |
24 hours |
7 days |
MAXIPIME Admixture Incompatibility
Do not add solutions of MAXIPIME, to solutions of ampicillin at a concentration greater than 40 mg per mL, or to metronidazole, vancomycin, gentamicin, tobramycin, netilmicin sulfate, or aminophylline because of potential interaction. However, if concurrent therapy with MAXIPIME is indicated, each of these antibiotics can be administered separately.
Intramuscular MAXIPIME
MAXIPIME constituted as directed is stable for 24 hours at controlled room temperature 20°C to 25°C (68°F to 77°F) or for 7 days in a refrigerator 2°C to 8°C (36°F to 46°F) with the following diluents: Sterile Water for Injection, 0.9% Sodium Chloride Injection, 5% Dextrose Injection, Sterile Bacteriostatic Water for Injection with Parabens or Benzyl Alcohol, or 0.5% or 1% Lidocaine Hydrochloride.
Intramuscular and Intravenous MAXIPIME
As with other cephalosporins, the color of MAXIPIME powder, as well as its solutions tend to darken depending on storage conditions; however, when stored as recommended, the product potency is not adversely affected.
ADD-Vantage Instructions for Reconstitution and Intravenous Administration
To Open
Peel overwrap at corner and remove solution container. Some opacity of the plastic due to moisture absorption during the sterilization process may be observed. This is normal and does not affect the solution quality or safety. The opacity will diminish gradually.
Assembly of Vial and Flexible Diluent Container
- 1.
- Use Aseptic Technique
- 2.
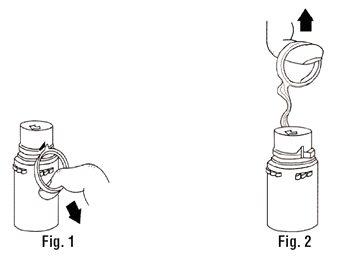
- Remove the protective covers from the top of the vial and the vial port on the diluent container as follows:
- a.
- To remove the breakaway vial cap, swing the pull ring over the top of the vial and pull down far enough to start the opening (See Figure 1), then pull straight up to remove the cap (See Figure 2)
- b.
- Once the breakaway cap has been removed, do not access vial with syringe.
-
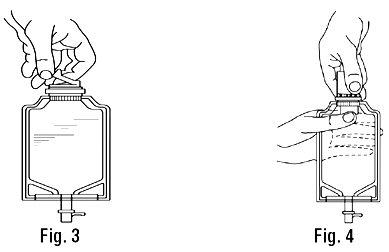
- c.
- To remove the vial port cover, grasp the tab on the pull ring, pull up to break the three tie strings, then pull back to remove the cover (See Figure 3.)
- 3.
- Screw the vial into the vial port until it will go no further. The Vial Must Be Screwed In Tightly To Assure a Seal. This occurs approximately 1/2 turn (180°) after the first audible click (see Figure 4). The clicking sound does not assure a seal; the vial must be turned as far as it will go. Once vial is seated, do not attempt to remove (See Figure 4).
- 4.
- Recheck the vial to assure that it is tight by trying to turn it further in the direction of assembly.
- 5.
- Label appropriately.
Instructions for Reconstitution MAXIPIME ADD-Vantage Vial in Flexible Diluent Container
- 1.
- Squeeze the bottom of the diluent container gently to inflate the portion of the container surrounding the end of the drug vial.
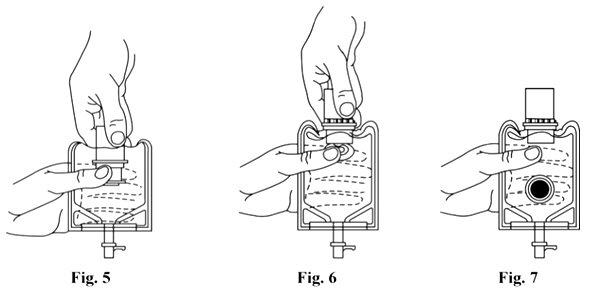
- 2.
- With the other hand, push the drug vial down into the container telescoping the walls of the container. Grasp the inner cap of the vial through the walls of the container (see Figure 5).
- 3.
- Pull the inner cap from the drug vial (see Figure 6). Verify that the rubber stopper has been pulled out, allowing the drug and diluent to mix.
- 4.
- Mix container contents thoroughly and use within the specified time [see Dosage and Administration (2.6)].
- 5.
- Look through the bottom of the vial to verify that the stopper has been removed and complete mixing has occurred (see Figure 7).
- 6.
- If the rubber stopper is not removed from the vial and medication is not released on the first attempt, the inner cap may be manipulated back into the rubber stopper without removing the drug vial from the diluent container. Repeat steps 3 through 5.
Instructions for Intravenous Administration of MAXIPIME ADD-Vantage Vial
- 1.
- Use Aseptic Technique
- 2.
- Confirm the activation and admixture of vial contents.
- 3.
- Check for leaks by squeezing container firmly. If leaks are found, discard unit as sterility may be impaired.
- 4.
- Close flow control clamp of administration set.
- 5.
- Remove cover from outlet port at bottom of container.
- 6.
- Insert piercing pin of administration set into port with a twisting motion until the pin is firmly seated. Refer to full directions on administration set carton prior to use.
- 7.
- Lift the free end of the hanger loop on the bottom of the vial, breaking the two tie strings. Bend the loop outward to lock it in the upright position, then suspend container from hanger.
- 8.
- Squeeze and release drip chamber to establish proper fluid level in chamber.
- 9.
- Open flow control clamp and clear air from set. Close clamp.
- 10.
- Attach set to venipuncture device. If device is not indwelling, prime and make venipuncture.
- 11.
- Regulate rate of administration with flow control clamp.
- 12.
- Do not use flexible container in series connections
More about Maxipime (cefepime)
- Check interactions
- Compare alternatives
- Side effects
- During pregnancy
- Drug class: fourth generation cephalosporins
- Breastfeeding
Patient resources
Professional resources
Related treatment guides
Further information
Always consult your healthcare provider to ensure the information displayed on this page applies to your personal circumstances.
